

Bladder Cancer Treatments, Surgeries, and Therapies
🔶 TUR / Transurethral Resection : Trans = by way of; urethral = urethra; This is usually done under general anesthesia (they put you to sleep for the surgery). A rigid cystoscope is used, along with resectoscope (see definitions below).
🔶
TURBT / Transurethral Resection of Bladder Tumor:
Trans = by way of; urethral = urethra; resection = to take out; bladder
tumor = a mass or tumor found in the bladder. It's a
surgery in which they remove a tumor in the bladder by going through the
urethra. This is usually done under general anesthesia (they put you to
sleep for the surgery). A rigid cystoscope is used, along with
resectoscope (see definitions below).
🔶 Resectoscope: A flexible instrument that can be inserted through the cystoscope sheath, or tube. The resectoscope has a wire loop that is used to remove the tumor. It also has a tool that uses an electric current to cut, remove, or destroy tissue and control bleeding. This is called fulguration.
🔶 Blue Light Cystoscopy:
It's a normal cystoscopy, but a special blue light on the end of the
cystoscope. This is a technology to detect and diagnose tumors in the
bladder. It
uses a
contrast solution that is absorbed by bladder cancer cells and makes
them turn
bright pink or red under a special blue light. This can be used during a
TURBT surgery, to find cancer cells that you human eye can't pick up
with just white light that is normally used with a cystoscopy. Some
doctors offices are also offering a blue light cystoscopy in their
offices. Many are not because of the increased expense for them. Many
insurance companies refuse to pay extra for a blue light cystoscopy.
🔶 Narrow Band Imagine Cystoscopy / NBI : A new technology that utilizes light of specific blue and green wavelengths. It's thought to improve the physician’s ability to detect small, non-muscle-invasive tumors that may not be seen with conventional cystoscopy. The technology takes advantage of the benefits of varying wavelengths of white light without the need for dyes or drugs. This can be done in the urologists office, or during a TURBT surgery.
🔶 Fulguration: Destroying tissue using
an electric current. This can be done during a cystoscopy, or during a
TURBT to destroy the bladder cancer.
🔶 Perforate / Perf / Perforation: Perforation
isa hole that develops thourgh the wall of a body organ like the
bladder. This can happen in surgery. If the bladder is perforated, then a
foley catheter is placed for several days, while the bladder whall
heals.
🔶 Resection / Excision: surgery to remove tissue or part or all of an organ
🔶 Incision: A cut made in the body during surgery.
🔶 BCG / Bacillus Calmette Guerin / Tice BCG: BCG is an active form of tuberculosis. Yes, you read that right. Tice BCG is a specific strain that is used in bladder cancer treatment. In the 1970's some scientists noticed that mice that had active tuberculosis, did not get cancer. Thus was born immunotherapy, a treatment that helps your immune system fight the cancer. BCG treatment is given to those with early-stage bladder cancer, stage 0 and stage 1. Those stages mean the cancer has not got into the muscle, and so it's called non-muscle invasive bladder cancer (NMIBC). BCG is instilled or inserted directly into the bladder, through a catheter (small flexible tube). BCG is the gold standard treatment used to treat early-stage bladder cancer. It is usually given once per week.
🔶 Immunotherapy / Cancer Immunotherapy / Biological Therapy / Biotherapy / Biological Response Therapy (BRM) : Treatment to stimulate or restore the ability of a person's immune system to
fight infection and disease. Also used to lessen side effects that may
be caused by some cancer treatments. There are many types of immunotherapy used with different treatments of bladder cancer. The most common type is BCG.
🔶 Catheter / Straight Cath / Self-Cath / Foley Catheter: a catheter is a narrow, flexible tube taht can be used to drain and collect urine from the bladder. It can also be used to infuse medication or fluid into the bladder. A regular catheter or straight catheter or the catheter used for self catheterization, is for a one time use only. A foley catheter has a balloon at the end of it. After the catheter is threaded into the urethra and then into the bladder, the ballon is inflated with saline. This catheter will stay in place for as long as needed. It does need to be periodically changed. The ballon stays inflated until the saline is taken out. The balloon keeps the catheter inside the bladder. A foley catheter might be used for many instances including after surgery if the bladder was perforated (a hole made in the wall), or if you can't urinate after BCG.
🔶 Maintenance BCG: The schedule of BCG includes an initial 6 weeks once per week, then 3 weeks (once per week) at 3 months, 6 months, 12 months, 18 months, 24 months, 30 months, and 36 months. All the doses of 3 weeks, are considered maintenance BCG doses.
🔶 Induction BCG: this the initial 6 weeks of BCG that are given after the TURBT. The BCG is given once per week.
🔶 Intravesical / Intravesical BCG / Intravesical Chemotherapy / Local Therapy: Local therapy is treatment that affects cells in the tumor and the area close to it. Intravesical therapy is a local therapy for bladder cacner. With intravesical therapy, the doctor puts a liquid drug right into your bladder rather than giving it by mouth or injecting it into your blood. The drug is put in through a soft catheter that's put into your bladder through your urethra. The drug stays in your bladder for up to 2 hours. This way, the drug can affect the cells lining the inside of your bladder without having major effects on other parts of your body. BCG, and chemotherapy are common medications used for intravesical therapy to treat bladder cancer.
🔶 Local Thearpy: Local therapy is treatment that affects cells in the tumor and the area close to it.
🔶 Systemic Thearpy: Treatment that uses substances that travel through the bloodstream, reaching and affecting cells all over the body.
🔶 Radiation / Radiotherapy / External Radiation / External-Beam Radiation: A cancer treatment that uses a machine to aim high-energy, high doeses of radiation rays at the cancer. Radiation therapy kills cancer cells, slows their growth by damaging their DNA, or will shrink cancer tumors.
🔶 Chemotherapy / Chemo: used to treat cancer as anti-cancer drugs. Often is cytotoxic (means that it damages or kills cells). Chemotherapy often is targeted for fast growing cells in your body. It can be given intravenously (IV, or in your vein), or intravesical (put directly into your bladder). That would include cancer, but unfortunately will also target your gut (thus the nausea and vomiting), as well as hair follicles, or the structures in the skin from which hair grows. Hair follicles are some of the fastest growing cells in the body.
🔶 Intravenous / IV :
a therapy in which medicaitons or fluids are given straight into your
vein. A device is put in your vein by inserting a needle into your skin,
and peircing the vein. The device will be taped and a dressing put over
it. This device is called an IV. How the medication is given is also
called IV or intravenous. For instance you will see written down Normal
Saline IV. That means that they normal saline will be given
intravenously.
🔶 Neoadjuvant / Neoadjuvant Therapy: Treatment given as a first step to shrink a tumor bofore the main treatment, which is usually surgery. Examples of neoadjuvant therapy include chemotherapy, radiation therapy, and hormone therapy. It is a type of induction (first or starting) therapy.
🔶 Adjuvant / Adjuvant Therapy: Additional cancer treatment given after the primary, or initial, treatment to lower the risk that the cancer will come back. Adjuvant therapy may include chemotherapy, radiation therapy, hormone therapy, targeted therapy, or biological/immunotherapy therapy.

Bladder Removal and Urinary Reconstruction Surgery Terms
🔶 Cystectomy / Complete Radical Cystectomy (RC) / Complete RC / Partial RC / Segmental Cystectomy: Radical means total or complete. Cystis means bladder, and ectomy means removal. So a complete radical cystectomy is the total surgical removal of the bladder. When a radical cystectomy is performed, your surgeon needs to reconstruct the urinary tract in one of three ways so that your urine can be eliminated from your body: illeal conduit, continent cutaneous diversion/pouch, and neobladder. Partial cystectomy or segmental cystectomy (they are the same thing) is pretty uncommon, in which with the tumor, only a part of the bladder would be removed. If you want a more detailed and excellent description of this process and options available please visit this website from Bladder Cancer Advocacy Network (BCAN).
🔶 Urinary Diversion / Incontinent Urinary Diversion / Urinary Reconstruction / Continent Urinary Diversion: Urinary diversions are surgical
procedures that create new ways for urine to exit your body. These need
to be done because the bladder and other structures are removed. There are three surgeries
that do this. They are called illeal
conduit, continent cutaneous diversion/pouch, and neobladder.
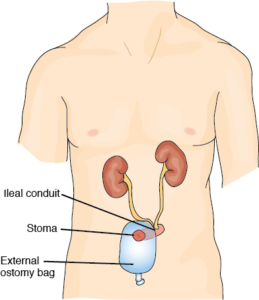
🔶 Ileal Conduit (IC): This is the easiest and most common reconstruction. Your surgeon disconnects a short portion of your small intestine called the ileum. One side of the piece of ileum is attached to a skin opening on the right side of the abdomen and a small stoma, or mouth, is created. A conduit or a passageway between the kidneys and ureters and the urethra is made using the piece of the intestine - the ileum. The ureters (tubes that carry urine from the kidney to the bladder) are attached to one end of the ileum, while the other end of the ileum is attached to the stoma. The stoma is usually located close to the belly button on the right side. A plastic appliance called an ostomy bag, is placed over the stoma to collect urine. Because the nerves and the blood supply are preserved, the conduit is able to propel the urine into the appliance, or ostomy bag.
🔶 Ostomy / Ostomy Bag / Stoma / Urostomy / Ostomate: A
stoma is an opening or pathway that your surgeon makes, from the inside
of your body to the skin on the outside of your body. A urostomy is a
stoma made for your urinary system - so you can get urine out of your
body when your bladder has been surgically removed. Your urine will
drain into a bag, or ostomy bag, that you put around your stoma. You’ll
drain the bag as
needed. This is created and used in an Illeal Conduit surgery. There is
also a stoma with the continent cutaneous diversion surgery, but there
is no bag on the outside to hold the urine. There is a pouch made inside
the body that a catheter will access to get the urine out. Someone who
has a stoma is called an ostomate.
🔶 Wound Ostomy Continence Nurse / WOCN Nurse / WOC Nurse / Enterostomal Therapist: a registered nurse that is specially trained to take care of ostomies, and to teach their patients how to manage them is called a wound ostomy continence nurse or WOCN nurse or WOC nurse. They might also help the surgeon figure out the best location for your stoma. An enterostomal therapist is a health professional trained in the care of persons with urostomies and other stomas.
🔶 RC/IC ; Radical Cystectomy With Ileal Conduit: This is the most common urinary system reconstruction. This is the removal of the bladder, with an illeal conduit reconstruction of the urinary tract. You will often see people write RC/IC.

🔶 Urinary Pouch: A urinary pouch is created from a continent cutaneous pouch surgery. You’ll put a drainage catheter (thin, flexible tube) into the stoma several times a day to drain your urine.

🔶 Neobladder / Neobladder-to-Urethra Diversion: another method of reconstructing your urinary system, after bladder removal. Your surgeon uses a long piece of small intestine to create a continent reservoir to store urine. The surgeon reconstructs the tubular shape of the intestine an crates a sphere. The ureters are attached to one end of the reservoir, and the other end of the reservoir is connected to the urethra, the tube that carries urine out of your body, so you can pass urine in a similar way to what you did before surgery. You empty your reservoir periodically by relaxing your pelvic muscles and tensing your abdominal (belly) muscles.
🔶 Anterior Pelvic Exenteration / Anterior Exteneration: This is the standard operation to remove organs from your urinary and gynecologic (female) systems. This includes the removal of bladder, urethra, uterus, cervix, ovaries, and the anterior or front wall of the vagina. This operation has recently been modified so the urethra can be preserved. In addition, patients of childbearing age may wish to discuss with their surgeon techniques for preserving the uterus and cervix during a cystectomy (removal of the bladder). Because the bladder and urethra have been removed, this means you’ll need a new place for urine to leave your body. Your surgeon will connect your ureters to a new urinary collection system called a urinary diversion or urostomy.



