|
| Stages of Bladder Cancer |
 | |||
| Grades of Bladder Cancer |
 |
| Names of Bladder Cancer |
3 Types of Bladder Cancer

Pathology, Pathologists, and Pathology Report

For a quick glossary of terms concerning bladder cancer and pathology, types, stages, and grades click here.
After your TURBT (Transurethral Resection of Bladder Tumor - the surgery to take out the tumor, read about it more here ), they will take your tumor and send it to pathology, or a lab, in which they will look very closely at the sample of your tumor, under a microscope, looking at the cellular level of the tumor cells and bladder cells surrounding the tumor. The physicians specifically trained to do this are called pathologists.
Please remember, that not only can you get a second opinion from a urologist or oncologist, you can also get a second opinion on your pathology. EVERYTHING concerning your treatment is about the pathology, so its vital that you understand what it is, and you are sure that the pathology is correct.
After the tumor or tissue sample has been identified and assessed, they will give your doctor a pathology report, that gives all the information about the tumor. This report will tell you if the tumor is cancer or not. If it is cancer then the report will tell you the type of cancer, the stage of cancer, and the grade.
Be sure to get a copy of your pathology report. Your physician will sit down with you and discuss the pathology report. You are not going to understand a lot of what is said, so it's important to have that report so you can later look up information on your own.
If the cancer is too large, or has spread too far, they might not be able to get all of it, and have to use chemotherapy and radiation to shrink the tumors. Sometimes they have to do multiple surgeries and biopsies to get all the tumors.
If the tumor has invaded the muscle wall (stage 2 and above) then you will most likely need to have your bladder removed. If you want some basic understanding and definitions of possible surgeries and treatments with bladder cancer, click here.
The pathologist will determine if there are clean margins in the tissue samples. This means that when a tumor is taken out, at the outer edge of where the tumor was, healthy tissue is removed also. They check to make sure there is a large chunk of healthy tissue taken out that was under the tumor, meaning that "they got it all," and all the cancer cells have been removed. If you have clean margins that will mean that that got out all of the cancer tissue.
If they didn't get clean margins, they will need to take you back into surgery to remove more of the tumor, and verify once again that they got clean margins.
If it's a benign tumor, that means that it's not cancerous. It only grows in one place and won't spread or invade other parts of your body. Benign tumors may grow large but do not spread into, or invade, nearby tissues or other parts of the body.
If the tumor is malignant, then it means that it is cancerous. It means that the tumor is an abnormal mass of tissue when cells grow and divide more than they should, or do not die when they should, and if not taken out, it will spread and invade all over your body. Malignant tumors can spread into, or invade, nearby tissues. They can also spread to other parts of the body through the blood and lymph systems. These tumors are also called neoplasms.
If it's cancer, they will tell you the type, the stage, and the grade of the tumor. I will explain what all of this means later in this article. Just stick with me. It will all make sense.
Most of us need to read, and re-read all of this information. It's a lot to process. Bookmark this page, and you can always come back to it when you need. You have got this. 💗
I would recommend bringing a loved one with you when you get the results of your pathology report. You might see written on a paper in black and white that you have cancer. No more time for denial. It might be right there in front of you. Believe me, it's quite the shock. Personally, when I heard the word cancer come out of my doctors mouth, I was not able to process anything else. It was almost like what you see in the movies. All the voices in the room become white noise, and I wasn't hearing what anyone was saying or processing it.
This is part of the first stage of grief - shock. Click here for an article about going through the 7 stages of grief when you are diagnosed with cancer. It's normal, it's expected, and it's important to give yourself plenty of time, space, and grace as you go through this experience. Lots of intense emotions are going to be flying around as you go through the different stages of grief. There is a lot of loss with bladder cancer.
Be sure the loved one knows what you need from them before you get to the doctors office. Tell them if you get bad news, it's going to be their job to ask questions (write them down before hand), and write the answers down.

Bladder Cancer Tumor Names
Three types of bladder cancer may form, and each type of tumor can be present in one or more areas of the bladder, and more than one type can be present at the same time:
- Papillary tumors stick out from the bladder lining on a
stalk. It grows into the hollow center of the bladder, away from the bladder wall, instead of deeper layers of the bladder wall. It looks like cauliflower, coral or a fern.
- Sessile tumors lie flat against the bladder lining. Sessile tumors are much more likely than papillary tumors to grow deeper into the layers of the bladder wall.
- Carcinoma in situ (CIS) is a cancerous patch of bladder lining, often referred to as a “flat tumor.” The patch may look almost normal or may look red and inflamed. Most of the time it looks reddish, flat, and velvety looking patches, and does not grow into the hollow part of the bladder. CIS is a type of nonmuscle-invasive bladder cancer that is of higher grade and increases the risk of recurrence and progression. At diagnosis, approximately 10% of patients with bladder cancer present with CIS.

Bladder Cancer Types
The type of bladder cancer depends on how the tumor’s cells look under the microscope. The 3 main types of bladder cancer are:
-
Urothelial carcinoma. Urothelial carcinoma (or UCC) accounts for about 90% of all bladder cancers. It also accounts for 10% to 15% of kidney cancers diagnosed in adults. It begins in the urothelial cells found in the urinary tract. Urothelial carcinoma is sometimes also called transitional cell carcinoma or TCC.Urothelial carcinoma (transitional cellcarcinoma) is the most common type of bladder cancer. Urothelial carcinoma starts in the urothelial cells. Urothelial cells are cells that line the inside of the bladder. Urothelial cells also line other parts of the urinary tract, such as the kidney, the ureters, and the urethra. People with bladder cancer may also
have tumors in these places. It is important that these other areas are also checked for tumors. This is often checked with a yearly or once every two years CT Scan. Click here for more information about that. -
Squamous cell carcinoma. Squamous cells develop in the bladder lining in response to irritation and inflammation. Over time, these cells may become cancerous. Squamous cell carcinoma accounts for about 4-5% of all bladder cancers. Squamous cell carcinomas have a higher chance of becoming invasive.
-
Adenocarcinoma. This type accounts for about 1-2% of all bladder cancers and develops from glandular cells. Adenocarcinomas of the bladder have a higher likelihood of being invasive at diagnosis.
There are other, less common types of bladder cancer, including sarcoma of the bladder and small cell bladder cancer, among others. Sarcomas of the bladder often begin in the fat or muscle layers of the bladder. Small cell bladder cancer is a rare type of bladder cancer that is likely to spread to other parts of the body.
What is Upper Tract Urothelial Carcinoma (UTUC)?
While the majority of bladder cancers (approximately 90-95%) arise in the bladder, the urothelial cells that line the bladder are found in other locations in the urinary system. Sometimes these urothelial cancers can occur in the lining of the kidney or in the ureter that connects the kidney to the bladder. This is known as upper tract urothelial cancer (UTUC) correspond to a subset of urothelial cancers that arise in the urothelial cells in the lining of the kidney (called the renal pelvis) or the ureter (the long, thin tube that connects that kidney to the bladder).
 | |
| Grade 1 Grade 2 Grade 3 |
What are the Grades of Bladder Cancer Tumor
Grade is expressed as a number between 1 (low) and 3 (high, i.e. G3); the higher the number the less the tumor resembles a normal cell. In lieu of numbers to grade a bladder cancer tumor, your doctor may refer to the tumor simply as low or high grade.
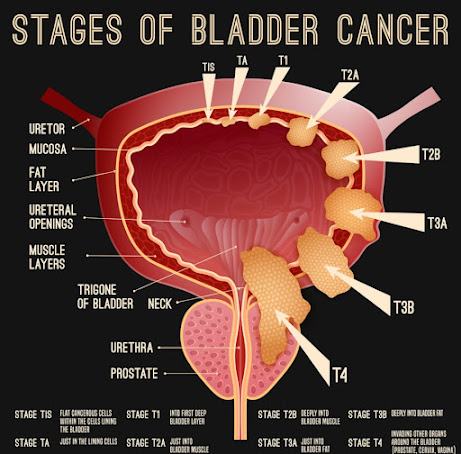
Stages of Bladder Cancer

Stage suggests the location of the tumor in relation to the inner lining of the bladder. The higher the stage the further the tumor has grown away from its original site on the surface. The following are the stages for bladder tumors:

- T0: No tumor
- Ta: Papillary tumor without invading the bladder wall
- TIS (CIS): Carcinoma in situ (non-invasive flat high-grade (G3) cancer)
- T1: Tumor invades the connective tissue under the surface lining
- T2: Tumor invades the muscle layer
- T3: Tumor penetrates the bladder wall and invades the surrounding fat layer
- T4: Tumor invades other organs (i.e., prostate, uterus, vagina, pelvic wall)
Stages of Bladder Cancer
One of the things you will learn from the pathology report is what stage the bladder cancer is.
A more simple way to understand staging is to think how large the tumor is, and how far it's grown into the bladder, or outside the bladder, and if it has spread to other parts of the body or lymph nodes.
After someone is diagnosed with bladder cancer, doctors will find out if it has spread, and if so, how far. This process is called staging. The stage of bladder cancer describes the extent or amount of cancer is in the bladder (or in the case of stage 4 how far it has grown out of the bladder). Staging is one of the most important factors in deciding how to treat bladder cancer and determining how successful treatment might be. It helps determine how serious the cancer is and how best to treat it.
To find the cancer’s stage, doctors try to answer these questions:
- How far has the cancer grown into the wall of the bladder?
- Has the cancer reached nearby tissues or organs?
- Has the cancer spread to the nearby lymph nodes or to distant organs?
The stage of bladder cancer is based on the results of physical
exams, biopsies, and imaging tests (CT, ultrasound, MRI, PET scan, x-rays, etc.), as well as the results of surgery or TURBT, in which the tumor and tissue samples are removed and sent to pathology for analysis. Click here if you want to review what a TURBT is.

Staging System
A staging system is a standard way for the cancer care team to describe how far a cancer has spread. The staging system most often used for bladder cancer is the American Joint Committee on Cancer (AJCC) TNM system, which is based on 3 key pieces of information:
- T describes how far the main (primary) tumor has grown through the bladder wall and whether it has grown into nearby tissues.
- N indicates any cancer spread to lymph nodes near the bladder. Lymph nodes are bean-sized collections of immune system cells, to which cancers often spread first.
- M indicates if the cancer has spread (metastasized) to distant sites, such as other organs, like the lungs or liver, or lymph nodes that are not near the bladder.
As a rule, the lower the number, the less the cancer has spread. A higher number, such as stage IV, means a more advanced cancer. Within a stage, an earlier letter (like a vs. b) means a lower stage. Cancers with similar stages tend to have a similar outlook and are often treated in much the same way.
Bladder cancer staging can be complex. If you have any questions about your stage, please ask your doctor to explain it to you in a way you understand.

Has the Tumor Invaded the Muscle Layer?
The
most important differentiation in the treatment of bladder cancer is if
it has invaded the muscle or not. The treatments are radically
different, and as you read information about bladder cancer, and discuss
this with others in bladder cancer groups and talk about it with your
doctor they will use the term "invasive" and "non-muscle invasive" and
"muscle invasive".
Please review the anatomy of the bladder layers above. Remember, in general terms the bladder is a really large muscle that stores urine for convenience, and also pushes out the urine when it's time to urinate or void.
The stages of bladder cancer is all based on which layer of the bladder, the tumor has invaded or grown into.
Noninvasive - stage 0 Noninvasive bladder cancer includes noninvasive papillary carcinoma (Ta) and carcinoma in situ (CIS). Noninvasive papillary carcinoma is a growth found on a small section of tissue that is easily removed. This is called stage Ta. CIS is cancer that is found only on or near the surface of the bladder, which is called stage Tis.
Non-muscle invasive bladder cancer - stage 0 and stage 1 (NMIBC - meaning it does NOT go into the muscle layer of the bladder) is the most common bladder cancer. I know it sounds weird using the word invasive. You have to focus on the "non-muscle" part of the term. This is the earliest stage of bladder cancer, and least invasive. It includes stage 0 and stage 1. About 90% of bladder cancers are non-muscle invasive, and are the most common type.
Muscle-invasive bladder cancer - stage 2, 3, and 4 is when the cancer has grown into deeper layers of the muscular bladder wall. These are more likely to spread to other organs and are harder to treat. This includes stages 2, 3, and 4. Often these stages will mean the removal of the bladder entirely (called a cystectomy, click here for some basic definitions and types of surgeries available).
It is important to note that non-muscle-invasive bladder cancer has the
possibility of spreading into the bladder muscle or to other parts of
the body. Additionally, all cell types of bladder cancer can spread
beyond the bladder to other areas of the body through a process known as
metastasis.
Stage 0 Bladder Cancer
Stage 0 bladder cancer is tumor found only growing in the very first layer, or lining of the bladder wall, called the urothelium layer or transitional epithelium. It has not grown into the connective tissue or muscle of the bladder. It has not spread to nearby lymph nodes (N0) or metastasized or spread to distant sites in the body (M0).
Nearly all bladder cancers start in the lining or urothelium. As the cancer grows into or through the other layers in the bladder, it becomes more advanced (the stage goes up).
There are many names that people use to describe cancer, and it can be really confusing. I have gathered all of these names into one place, and described what all the letters and words mean. Click here for that basic list with definitions. I will go into greater detail below, about what all of it means.
There are two main types of stage 0 bladder cancer: Ta and CIS
 |
| Ta Tumor |
Ta / non-invasive papillary carcinoma / noninvasive / stage Ta / Ta0 / papillary transitional cell carcinoma / TCC (see above picture)
- One type of stage 0 bladder cancer
- The "T" stands for tumor
- The "a" means its in the very early stages of cancer
- The "0" stands for stage zero
- Non-invasive means it's not in the muscle, remember stage 0 means it's only in the very first layer, or lining of the bladder wall, called the urothelium layer or transitional epithelium.
- Papillary is the description of what it looks like. It grows into the hollow center of the bladder and looks like cauliflower, coral or a fern.
- Transitional Cell Carcinoma is just meaning the location of where it is. This bladder cancer forms in the first layer of the bladder wall called the urothelium layer or transitional epithelium layer.
- Also called Non-muscle invasive bladder cancer (NMIBC) : it has not invaded the muscle wall of the bladder
- Also called Superficial bladder cancer: it's only on the first layer of the bladder wall
- Also called Non-invasive carcinoma: it has not invaded the muscle wall of the bladder
- Also called Urothelial carcinoma / transitional cell carcinoma (TCC):
transitional and urothelial cells are in your urinary system. They are
part of the transitional epithelium layer or urothelium layer. This
layer lines the bladder, ureters, urethra, and kidneys. This is why a
yearly CT needs to be done when you have bladder cancer. It can spread
to other areas of the urinary system.
 |
| CIS or Carcinoma in situ Tumor |
CIS / Tis / CIS0 / Tis0 /stage Tis / stage 0is / carcinoma in situ (in SY-too) / non-invasive carcinoma / urothelial carcinoma in situ / flat carcinoma in situ (see above picture)
- One type of stage 0 bladder cancer
- The "T" stands for tumor
- The "C" stands for carcinoma which is cancer that forms in the urothelium layer or transitional epithelium of the bladder. This is the first layer of the bladder wall.
- The "is" stands for in situ (in SY-too), which means in its original place. So the cancer cells are only found in the layer they first formed and has not spread further, which for bladder cancer means the lining of the first layer of the bladder wall, called the urothelium layer or transitional epithelium.
- Non-invasive means that it has not invaded the muscle layer of the bladder
- Description of CIS: This type of cancer is reddish, flat, and velvety looking patches, and does not grow into the hollow part of the bladder.
- CIS is high grade: This is a high grade cancer (also called grade 3). I will talk more about grades later on. What this means is that although CIS is a stage 0 cancer, it is high grade, which makes it more aggressive, with a tendency toward progressing to higher bladder stages. It has increased chances of coming back again. It is harder to cut all of it out, because it's harder to see.
- Also called Non-muscle invasive bladder cancer (NMIBC) : it has not invaded the muscle wall of the bladder
- Also called Superficial bladder cancer: it's only on the first layer of the bladder wall
- Also called Non-invasive carcinoma: it has not invaded the muscle wall of the bladder
- Also called Urothelial carcinoma / transitional cell carcinoma (TCC):
transitional and urothelial cells are in your urinary system. They are
part of the transitional epithelium layer or urothelium layer. For some reason a CIS tumor is rarely called a transitional cell carcinoma. Usually that term is associated with a Ta tumor. This
layer lines the bladder, ureters, urethra, and kidneys. This is why a
yearly CT needs to be done when you have bladder cancer. It can spread
to other areas of the urinary system.

Stage 1 (T1, N0, M0) Bladder Cancer
Stage 1 bladder cancer has grown through the urothelium/transitional cell layer and grown into or invaded the lamina propria layer of the bladder wall. The lamina propria is also called the submucoa, and is a thin layer of connective tissue. This layer contains blood vessels, nerves and glands.
Stage 1 bladder cancer has NOT reached the muscle layer of the bladder. It has not spread to nearby lymph nodes (N0) or metastasized or spread to distant sites in the body (M0).
Just like stage 0, stage 1 bladder cancer is also called non-muscle invasive bladder cancer (NMIBC), meaning it has not invaded the muscle wall of the bladder.

Stage 2 (T2; T2a; T2b, N0, M0) Bladder Cancer
The cancer has grown into the inner (T2a) or outer (T2b) muscle layer of the bladder wall, but it has not passed completely through the muscle to reach the layer of fatty tissue that surrounds the bladder.
The cancer has not spread to nearby lymph nodes (N0) or to distant sites (M0).
This is muscle invasive bladder cancer. Most of the time stage 2 or higher bladder cancer will mean eventual removal of the bladder. Click here for a list and definitions of bladder cancer treatments, surgeries, and therapies.

Stage 3 Bladder Cancer
Stage 3A
- T3a, T3b, or T4a, N0, M0:
The cancer has grown through the muscle layer of the bladder and into the layer of fatty tissue that surrounds the bladder (T3a or T3b).
It might have spread into the prostate, seminal vesicles, uterus, or vagina, but it's not growing into the pelvic or abdominal wall (T4a).
The cancer has not spread to nearby lymph nodes (N0) or to distant sites (M0).
- T1-4a, N1, M0:
The cancer has grown into the layer of connective tissue under the lining of the bladder wall (T1), OR into the muscle layer of the bladder wall (T2), OR into the layer of fatty tissue that surrounds the bladder, (T3a or T3b) OR it might have spread into the prostate, seminal vesicles, uterus, or vagina, but it's not growing into the pelvic or abdominal wall (T4a).
AND the cancer has spread to 1 nearby lymph node in the true pelvis (N1).
It has not spread to distant sites (M0).
Stage 3B
- T1-T4a, N2 or N3, M0:
The cancer has grown into the layer of connective tissue under the lining of the bladder wall (T1), OR into the muscle layer of the bladder wall (T2), ORinto the layer of fatty tissue that surrounds the bladder (T3a or T3b), OR it might have spread into the prostate, seminal vesicles, uterus, or vagina, but it's not growing into the pelvic or abdominal wall (T4a).
AND the cancer has spread to 2 or more lymph nodes in the true pelvis (N2) or to lymph nodes along the common iliac arteries (N3).
It has not spread to distant sites (M0).
Stage 4 Bladder Cancer
Stage 4A
- T4b, any N, M0:
The cancer has grown through the bladder wall into the pelvic or abdominal wall (T4b).
It might or might not have spread to nearby lymph nodes (Any N).
It has not spread to a distant sites (M0)
- T4b, any T, any N, M1a:
The cancer might or might not have grown through the wall of the bladder into nearby organs (Any T).
It might or might not have spread to nearby lymph nodes (Any N).
It has spread to distant lymph nodes (M1a).
Stage 4B
- Any T, any N, M1b:
The cancer might or might not have grown through the wall of the bladder into nearby organs (Any T).
It might or might not have spread to nearby lymph nodes (Any N).
It has spread to 1 or more distant organs, such as the bones, liver, or lungs (M1b).